A Pre-Jaw Surgery Experiment
I have decided to run an experiment to see if I myself am a candidate for double jaw surgery.
For the next several weeks, until October 1, I am going to mimic post-jaw surgery anatomy by sticking my tongue out as I go about my daily activities.

If this results in a significant improvement of my headache symptoms, then I am going to commit to pursuing jaw surgery for the purpose of permanently giving me more tongue space.
You’re Having Headaches Again?
As many of my subscribers know, I have had a bad summer of headaches. The worst in many years.
Almost every other day for the past few months, I have been incapacitated with headache pain centered on the back of my neck that radiates to my eyes and temples, and causes lots of burping and indigestion. My symptoms jive with a diagnosis of occipital neuralgia.

And this has resulted in inconsistency of YouTube posting, as well as delaying the writing and publication of parts 5 and 6 of the JawHacks ebook.
Now that I have a wife, a 10 month old daughter, and another baby to be born in March, I simply cannot afford to be a slave to these headaches.
When I was living in a Sprinter, the pain sucked but at least the fallout was contained to me alone. However it’s not just about me anymore.
Headache Hypothesis
I have a working hypothesis that the reason I continue to get headaches is because of my tongue being cramped inside my mouth, like a folded accordion.
The posterior part of my tongue being kinked back is causing excessive pressure on the muscles at the back of my neck, causing those muscles to strain and impinge my lesser occipital nerves on both sides.

I have been meditating on the phenomenological experience of having my distinct type of headache, and two nights ago I made an important (re)discovery.
I call it a re-discovery because it’s actually something I figured out 10 years ago, which drove me to seek jaw augmentation in the first place.
And that realization is that when I allow my tongue to relax and fall forward out of my mouth, outside of my teeth, the tension in my neck immediately releases.
For example, last night while doing my evening workout/stretching, I switched back and forth between doing pull-ups with my tongue in (and my teeth gently together), and then with my tongue flopping out about a centimeter in front of my teeth.
It was unmistakable that the tongue-out pull-ups were much easier, involving almost no neck tension at all. And as soon as I bit my teeth gently together, forcing my tongue back into its “normal” retracted position, I could feel the occipital neuralgia symptoms percolating.
I did the same with dips, and then seated meditation, and then reading my Kindle on the couch. And the next morning I went for a short jog, also with my tongue out.
In all instances, releasing my tongue forward out of my mouth resulted in being able to engage with these activities with none of the usual neck pain.
But Didn’t MSE Fix My Headache Problem?
This tells me that maybe the root problem of my remaining headaches is the fact that I never achieved forward advancement of my jaws.
Yes, I expanded transversely with MSE back in 2019, and at that time I did experience a profound improvement in my headache symptoms. To this day, my headaches are much better (even at their worst) than they were prior to MSE.
As of recently, my headache frequency has been high (equal to my worst periods from the pre-expansion, pre-migraine surgery era of 2018-2019).
However, their severity and duration are down.
Before, my typical headache was a 7/10 or 8/10 with nausea and vomiting. Now my headaches are 4/10 with no vomiting. And they are easily aborted with triptan medications.
However, having a 4/10 headache multiple times per week is still a terrible nuisance and is preventing me from being as present and functional for my wife and daughter as I need to be. And of course, the financial pressure on me is at an all-time high.
So I really have no choice but to keep hunting down this headache problem and trying to put another big dent in it.
The MSE helped decompress my tongue somewhat, and did improve my symptoms. But I never actually achieved jaw advancement. Maybe that’s what’s missing for me.
If I could do a double jaw surgery, and allow my tongue to permanently park ~1cm farther forward than where it is now, maybe that nagging pressure in the back of my neck will be forever relieved.
Due Diligence Before Jaw Surgery
I am currently in my 9th straight year of orthodontic treatment (not including my 2 years of childhood extract and retract ortho).
And to say I am suffering from orthodontic burnout is an understatement. Since July 2016, I have had failed tooth-borne expansion, an MSE, Invisalign, regular braces, BRIUS lingual braces, Invisalign again, SFOT, and now more Invisalign.
My teeth are in rough shape and my mouth and mind have been through a lot.
And so now I am supposed to pony up and do a double jaw surgery, one of the scariest elective procedures on the planet?
It would be a travesty for me to do the jaw surgery and have no relief of the underlying headache condition. So I need to have some assurance that my “cramped tongue causing neck pressure” theory is not totally kooky.

Toward this end, I am going to run my tongue-out experiment for the next month. If I can reduce my headaches and neck pain over this period, I will strongly consider requesting the services of one of my jaw surgery colleagues.
Limits of My Experiment
Of course, sticking the tongue out of the mouth doesn’t perfectly mimic jaw surgery. To begin with, it’s very uncomfortable as the teeth bite into it. And that also puts excess pressure on the front teeth, which is not ideal for me, given my orthodontic history.
And it’s not possible to eat or talk with the tongue out, so those two activities will inevitably pull be back into the kinked-tongue / strained-neck position.
And then there’s the elephant in the room — sleep. I can’t sleep with my tongue out either, and so each night my experiment will be shut down, and bad things will probably happen to my neck while I am unconscious.
But I hope I can gather enough data during the day to be able to make a confident decision about jaw surgery.
My Chiari 1 Malformation
You may be wondering: “Ron – if you’re theory is correct, why doesn’t everyone with small jaws experience occipital neuralgia and chronic headaches like you?”
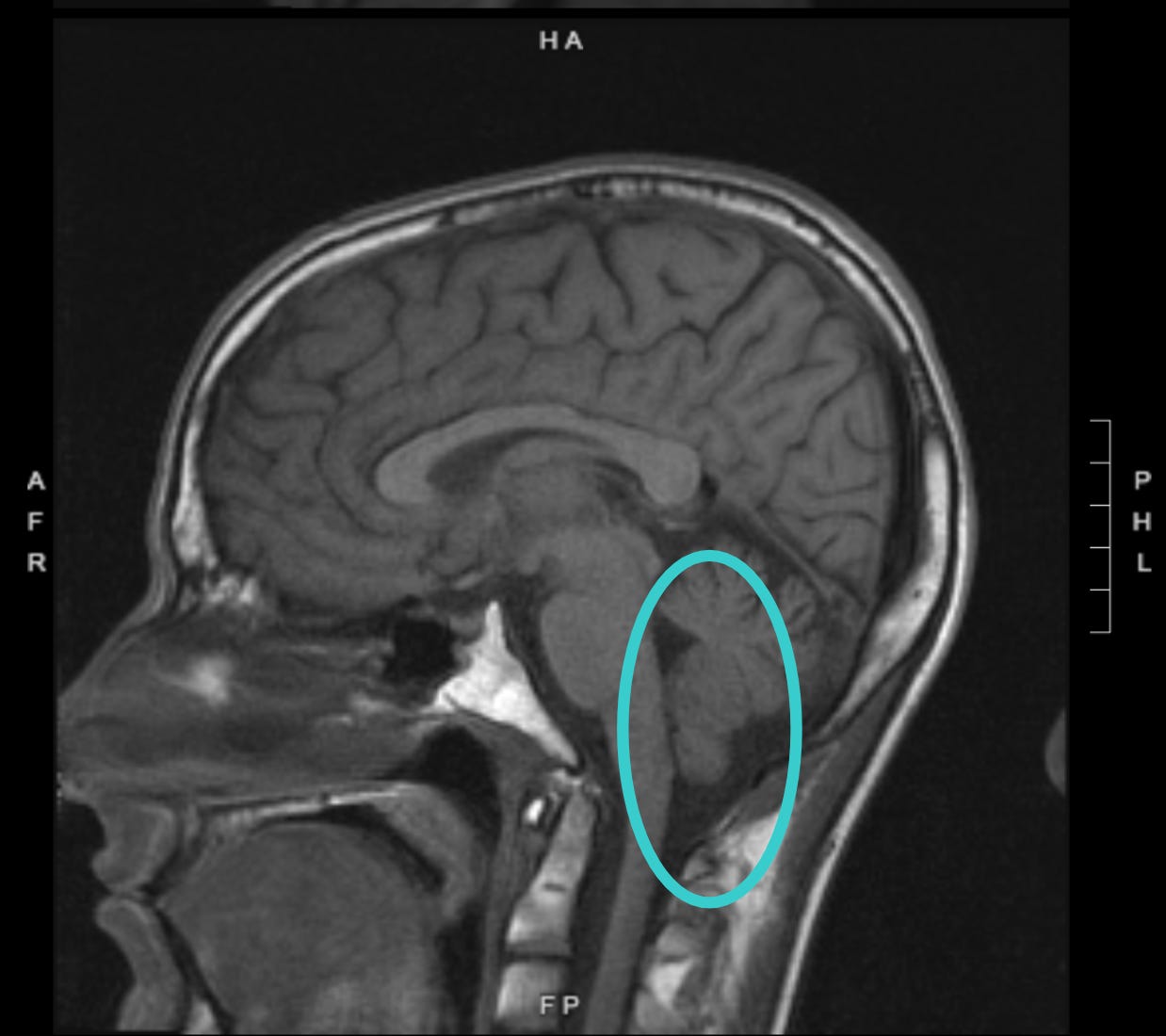
It’s possible that the key feature in my case is my Chiari 1 malformation. This is something I was diagnosed with back in 2011, but never really gave much thought until this year’s exceptionally bad summer of headaches.
A Chiari malformation is sort of like small jaws, but at the back of the skull. It is an underdevelopment of the back of the skull which results in a traffic jam of the cerebellum and the brain stem as they emerge from the foramen magnum, which is the hole at the base of the skull.

My Chiari malformation is not severe, but that doesn’t really mean much. As with sleep testing and sleep apnea, there is not a 1:1 relationship between AHI and severity of symptoms.
Similarly with Chiari, a small compression can be very symptomatic for some patients, and that may be the case with me, especially since I am a notoriously sensitive person.
My current theory is that the Chiari malformation is causing a central compression of my occipital nerves and other nerves of my neck and upper back, resulting in these nerves being “on edge” all the time.
By “central compression,” I mean that the nerve impingement is occurring at or very near to the brain stem and spinal cord as they emerge from the foramen magnum.
Since the nerves are already on edge, the excess muscular pressure and strain at the back of my neck being caused by my kinked tongue is causing these nerves to boil over, resulting in occipital neuralgia.
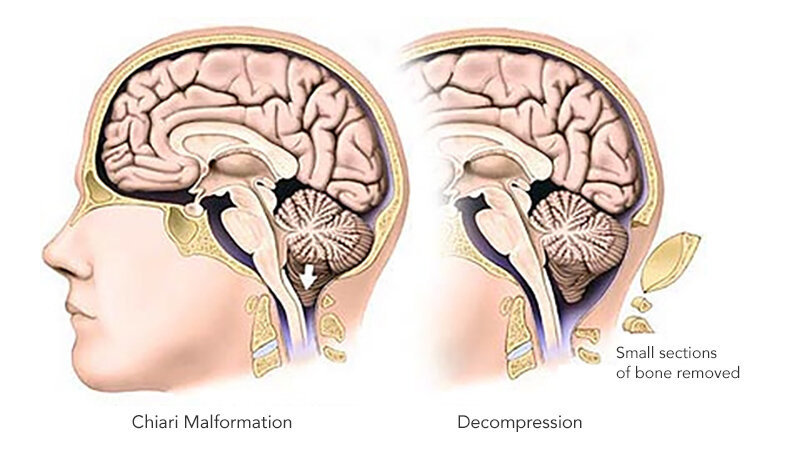
What About a Chiari Decompression Surgery?
The primary symptom of a Chiari malformation is constant cervicogenic headache, just like what I have. And many Chiari patients describe an experience that mimics that of occipital neuralgia patients, just like me.
So why not treat the Chiari malformation instead of the jaws? There is such a thing as a Chiari decompression surgery, in which a part of the skull is removed in order to relieve pressure of skull/brain/brainstem traffic jam previously described.
Whether or not I proceed with Chiari decompression will depend on the success of my tongue experiment this next month.
If I find that decompressing the tongue allows for my Chiari malformation to become asymptomatic again, then I would rather not do the very invasive neurosurgery involved in Chiari decompression which results in surgical exposure of the brain.
Doing the jaw surgery as opposed to the Chiari decompression also affords airway benefits. If I do the jaw surgery, and my headaches are still bad, at least I might have gained the ability to sleep on my back without choking (currently I struggle to breath in supine).
Are the Headaches Caused by Diet, Lifestyle and Stress?
It’s true, in some ways as a new husband and dad, I am more stressed than ever. For example, my sleep is very interrupted, and my morning fitness routine which I have long depended on for health stability is often disturbed by parenting duties.
But stress is definitely not the whole story here. I would tell you if it were, I’m not ashamed to admit to my mental susceptibility to the difficulties of life.
And with regards to diet, I went strictly carnivore about 3 weeks ago, and while symptoms have been reduced, there is still this distinct, localized pain in my neck that must have a mechanical source.

Additionally, I quit nicotine, cut way back on caffeine to one cup of tea per day, and use no other illicit drugs. I simply don’t know what else I could do to purify my biochemistry and lifestyle.
I have also tried to eliminate the sleep disordered breathing variable by returning to my old practice of sleeping with a backpack filled with balloons to force me to sleep on my side, where I never snore and choke.
If you have any other lifestyle suggestions that I should try prior to jaw surgery, please comment below.
What About My Migraine Nerve Decompression Surgeries?
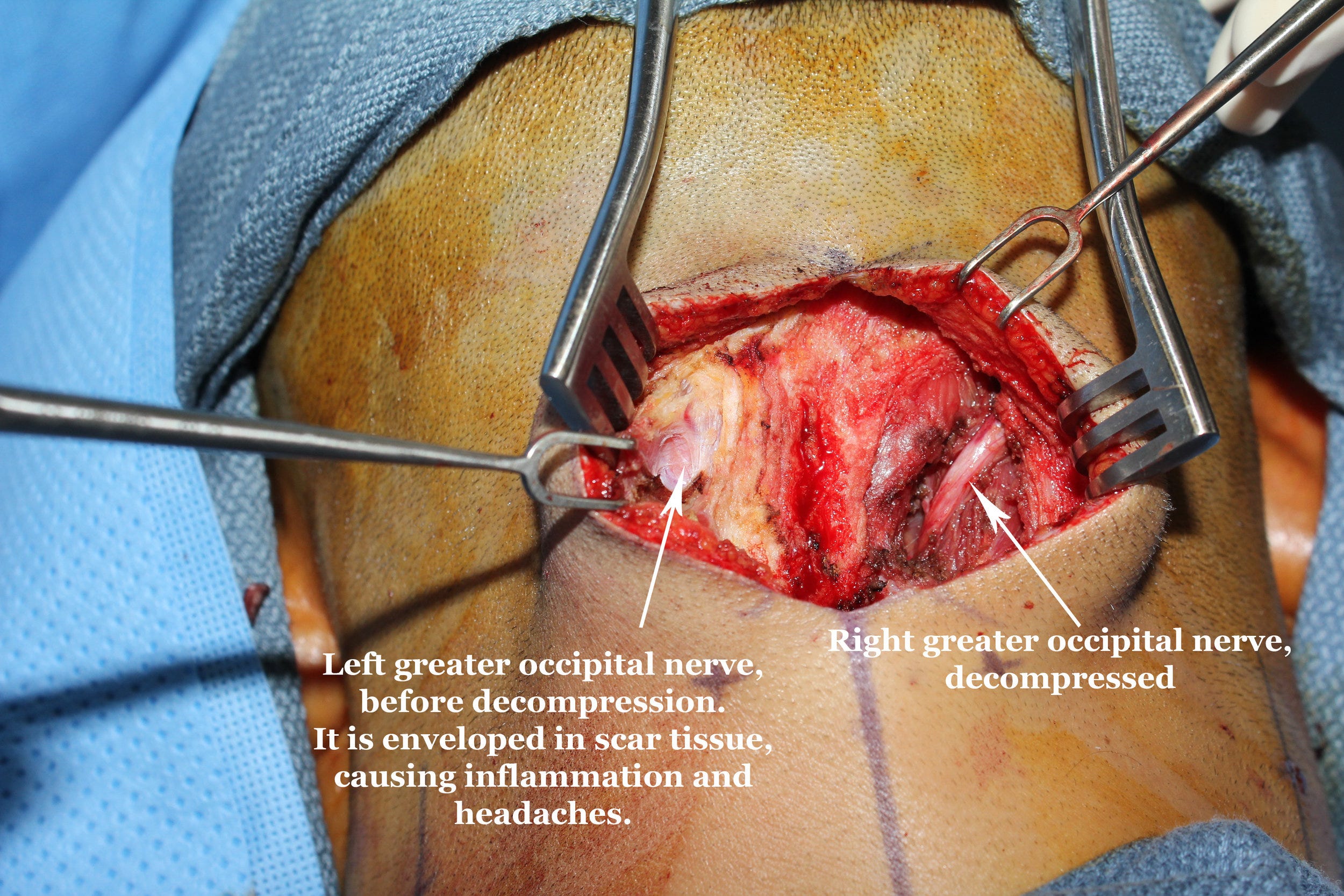
Yes, I have had three migraine nerve decompression surgeries. An initial surgery in December 2017 with Dr. Ziv Peled to excise the lesser and third occipital nerves, and decompress the greater occipital nerve.
A second surgery in April 2018 with Dr. Peled to decompress or excise the nerves in my eyebrows, temples and forehead.
And then a third surgery in January 2021 with Dr. Jay Austen to further investigate residual pain I was having in the area of my right lesser occipital nerve.
These surgeries were all helpful and definitely contributed to the enduring reduction in my headache severity.
But I believe what is happening now is that the nerves are being re-compressed by the excessive pressure being caused by my cramped tongue, likely the same pressure that has been compressing them since my childhood.
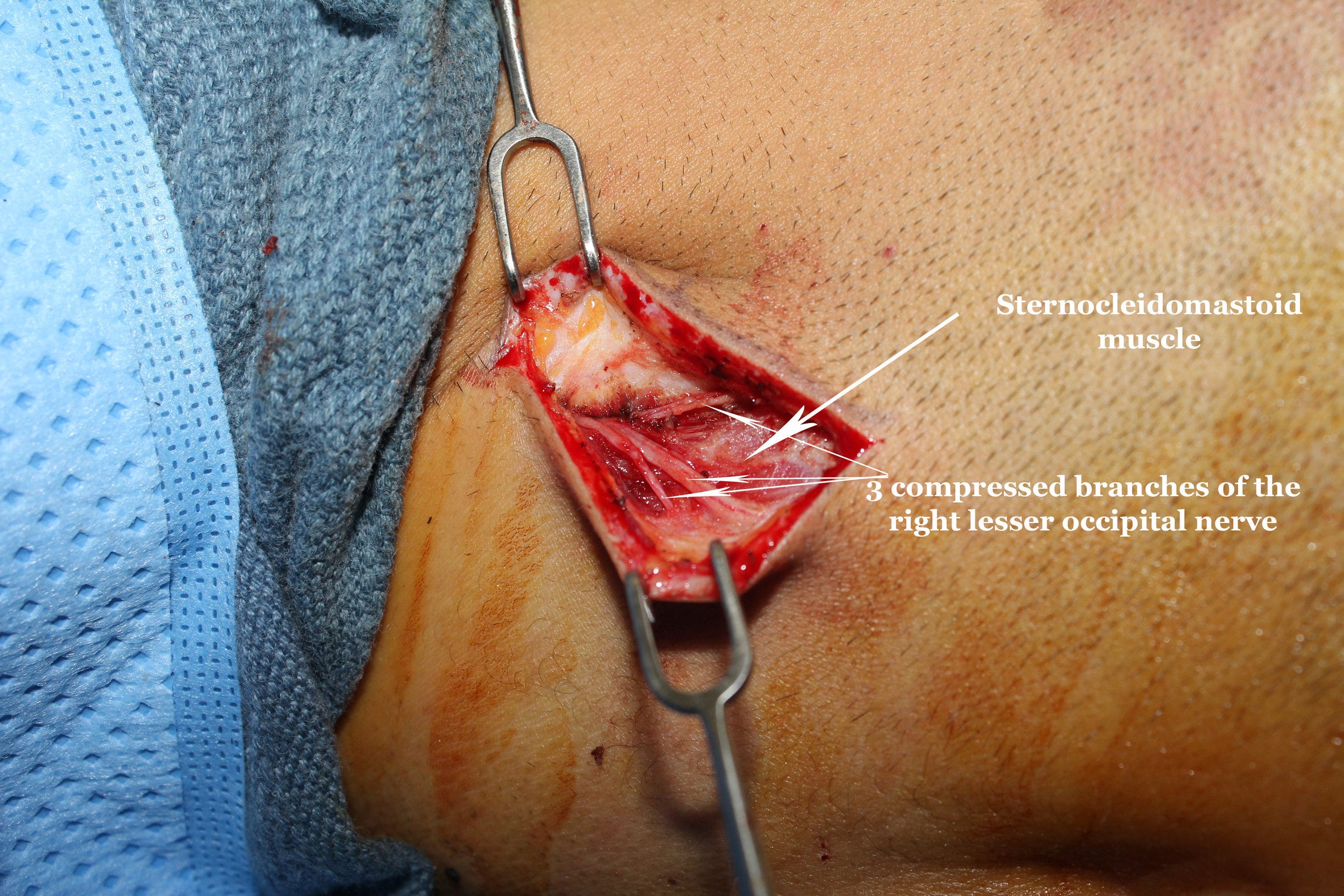
And in the case of my excised lesser occipital nerves (on both the left and right sides of my neck), I believe the nerve stubs that remained after Dr. Peled cut them are being irritated in the muscle where they were buried.
In fact, most of my current neuralgia pain occurs at the sites of my excised lesser occipital nerves, and I believe that those nerve stubs are directly irritated by the muscular pressure caused by my cramped tongue.
Fat Grafting for Nerve Pain?
If I do the jaw surgery and get a major improvement of my headache symptoms from the tongue decompression, but I still have some small amount of residual pain around the lesser occipital nerves, I would consider going back to Dr. Peled to do fat-grafting on these lesser occipital nerve stubs.

The fat grafting provides cushioning of the nerve, protecting it against the surrounding muscle. It also introduces stem cells to the area which could promote much needed healing of those nerves.
This fat grafting procedure would be like icing on the cake of this whole experimental headache treatment process.
Stay Tuned
That’s it for now. I will let you know how the “tongue-out” experiment progresses over the next month.

