Below is a lightly edited transcript from the talk by Dr. Zubad Newaz, DDS at MewCon 2024 on August 17. All images shown below are from Dr. Newaz’s MewCon 2024 slideshow.
Facial Structure and Health
I know it’s end of the day, everybody’s looking to get socializing again. So I’ll try to keep this as brief as I can.
Basically all of us here have something in common. I think we’re all asking certain kinds of questions that are not typically asked and we’re all here because, by definition, we claim not to know all the answers.
This is a oft evolving profession, and just like Mike [Mew] said at the very beginning, we’re just scratching the surface, right?
We’re here because we all share an appreciation for making the box bigger.
And the box is so important because it is the framework that houses and fits the tongue, the lower jaw, the airway…and our whole facial structure is the underpinning of good health and good function.
And I think we believe that, and it’s very important not to be dogmatic in any of our approaches on how to achieve that. Medicine is very individualized, and maintains the view as a community that one particular type of treatment modality is not for everybody.
So see what I’m presenting today as merely one of the tools in the toolbox to help “make the box bigger.”
Dr. Newaz Had Extractions
I’m here on this stage today because my own experiences have shaped me into what I’m doing now.
I had extraction orthodontics as a teenager. And by all orthodontic standards, I think my treatment was done very well. And then, of course, I started seeing different kinds of disturbances. Thankfully, I’m not suffering as much as many, but I still do feel the progression decade after decade, of the downstream effects of some of these things.

Dr. Newaz Getting His Own FME?
We may be starting the project to reverse that tomorrow. My partner may be installing [an FME] in my mouth. I’m very excited about that. And it’s good to know what you’re doing to people.
Dr. Newaz’s Training as a Oral Maxillofacial Radiologist
My own experience with orthodontic treatment was one thing, and then the other is before I became an orthodontist, I was a oral and maxillofacial radiologist, and I continue to practice that.
I really enjoy that part of the profession, because it is what connected me to people’s airways and diagnostic questions on a level that I was not otherwise trained as a clinician to do. So I feel like it’s been very helpful for me in this particular space to have the diagnostic background as well as a clinical background.
Dr. Newaz is New to Social Media
Some of you can know that I run a very inefficient business because I travel between three states. And also I have been brought onto the social media wagon by my beloved colleagues [Dr. Jaffari], and Bailey who’s somewhere lurking in the shadows here.
They both got me. I’m very shy, not public facing. So it has been good to start to get some of our message out there in ways that we try to do everyday with our patients.

Jaw Structure and The Central Nervous System
Everything that’s on this slide is pretty much the same thing that’s been repeated every lecture today, right? We’ve been talking about the box and some structural generalities about the jaws and the airway and so forth.
And I think it’s all about these last two things. We’re trying to improve the anatomic constrictions that contribute to airway compromise.
We know that there are a lot of those types of constrictions in the area, and we’re all trained to treat the diagnosis. And we are looking to improve the freedom from the mandible, and hence the tongue, the mandible itself and the joint associated with it.
The central nervous system doesn’t tend to like when things are compressed, there are a lot of intricate nerve endings and things like that in our face. And when the structures are constricted…we had a great talk this morning by our osteopathic physician [Dr. Tasha Turzo] about the role of the central nervous system in these kinds of issues. And again, how all that stuff relates…we don’t even claim to know the beginning of it. We just know that it does relate.
I think we will find out a lot more in this 22nd century of medicine, where we now are going to have all kinds of modeling and computerized data that we’re going to crunch, and as a community, we are going to have the answer to our contrarians, because that’s what we need, so that we’re not seen as a fringe.
We want this to be what is normal, what is the future of medicine.
Dr. Newaz on Myofunctional Therapy and Tongue Posture
While stability of expansion has been studied and reported in the literature, there is little to no emphasis in the profession and in the research about the role of tongue posture reeducation and optimization as it specifically pertains to holding expansion (and general orthodontic) results.
I give most of my patients a simple myofunctional regimen or guidance and if more sophisticated training is needed, I refer them to a myofunctional therapist.
And all studies right now that comment on the the efficacy and stability of expansion fail to mention tongue posture as a possible biomodulator. Not a single study today mentions that. And when you have the very scaffold that has been mentioned in all of these talks we have heard today, housing and supporting the structures of the face, it is senseless to make any conclusions without looking at that.
How in the world does anyone think expansion is going to be stable in the long-term if the tongue is not acting as a scaffold against the palate to hold and protect it?
Evolution of Bone Anchored Expanders
So we’ll talk a little bit about some of the evolution and different varieties of bone-anchored expanders. A lot of you are familiar with these designs already.
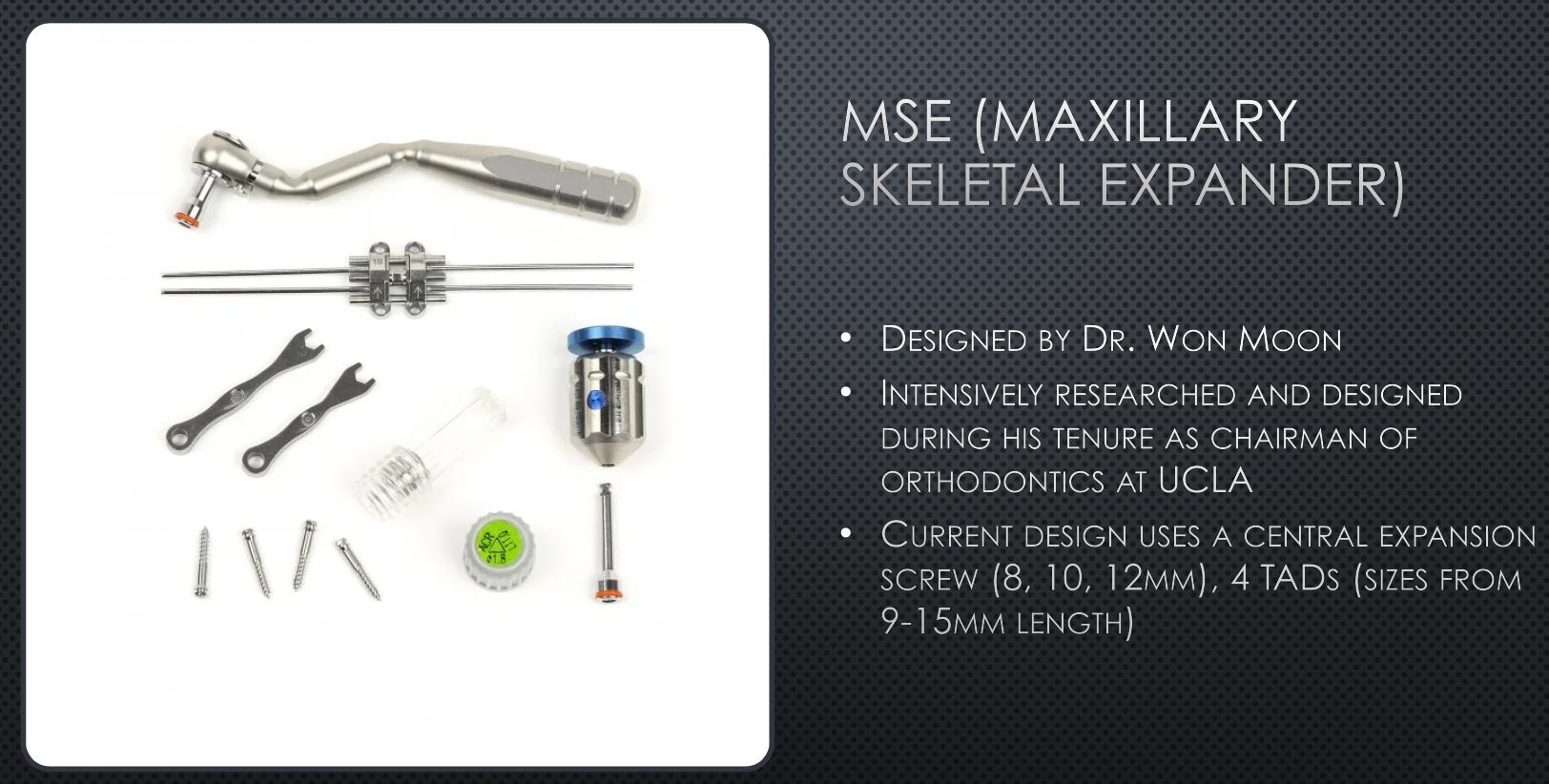
Credit to Dr. Won Moon, Intro to MSE
Lots of credit to Dr. Won Moon who has popularized and made it easy, reduced the barrier to entry, for those of us who are interested in having a solution to expand our patients’ maxillas, especially those who were either in a later stage of growing or non-growing.
(Because we have a lot more latitude and lot more options in growing patients than we do in non-growing patients.)
So this was a boon to those of us who felt we had our hands tied behind our backs without a relatively easy way to address it.
You’ll see some of the components of that particular expansion system here [MSE type 2].
[The below photos] are showing the concept of bone anchored expansion, and the skeletal effects it can have. We’re splitting not only the mid-palatal suture, but we’re also targeting other circummaxillary sutures higher up than simply just the mid-palatal suture.
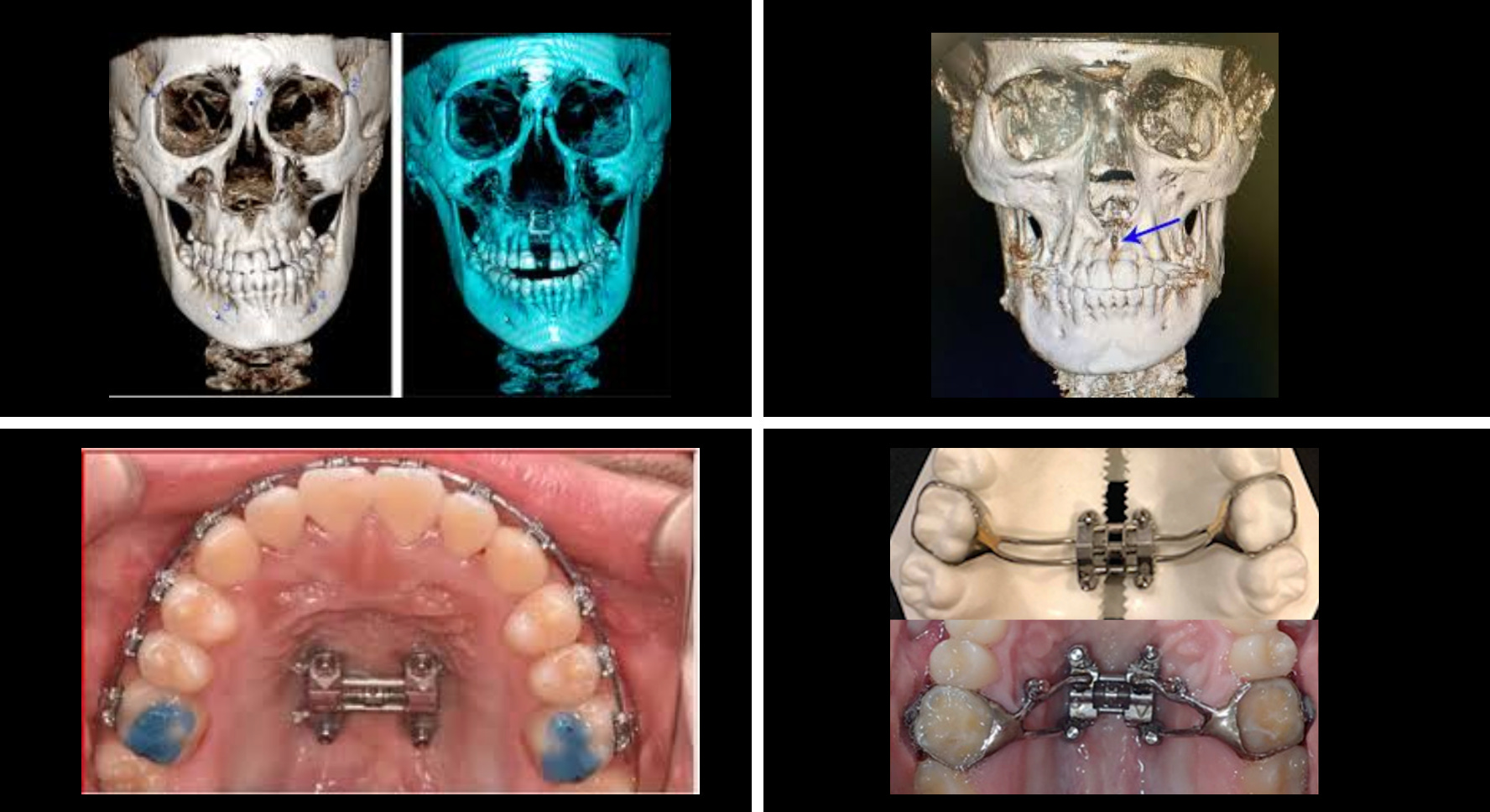
10 years ago, the only way you could expand an adult palate would be to go to the operating room and have an osteotomy, the same kind of cuts that Ronny [Ead] was talking about for purposes of moving the jaw forward.
We would have to make similar cuts, along with a midline cut to be able to skeletally expand an adult palate. That is no longer necessary.
Case Studies and Patient Transformations
And this is a quick smile photo of a patient that had done some standard MSE and Invisalign. You can kind of see how some tension was relieved in the face.
The smile is a little bit more relaxed. The area under the eyes looks a bit more relaxed and not retruded.
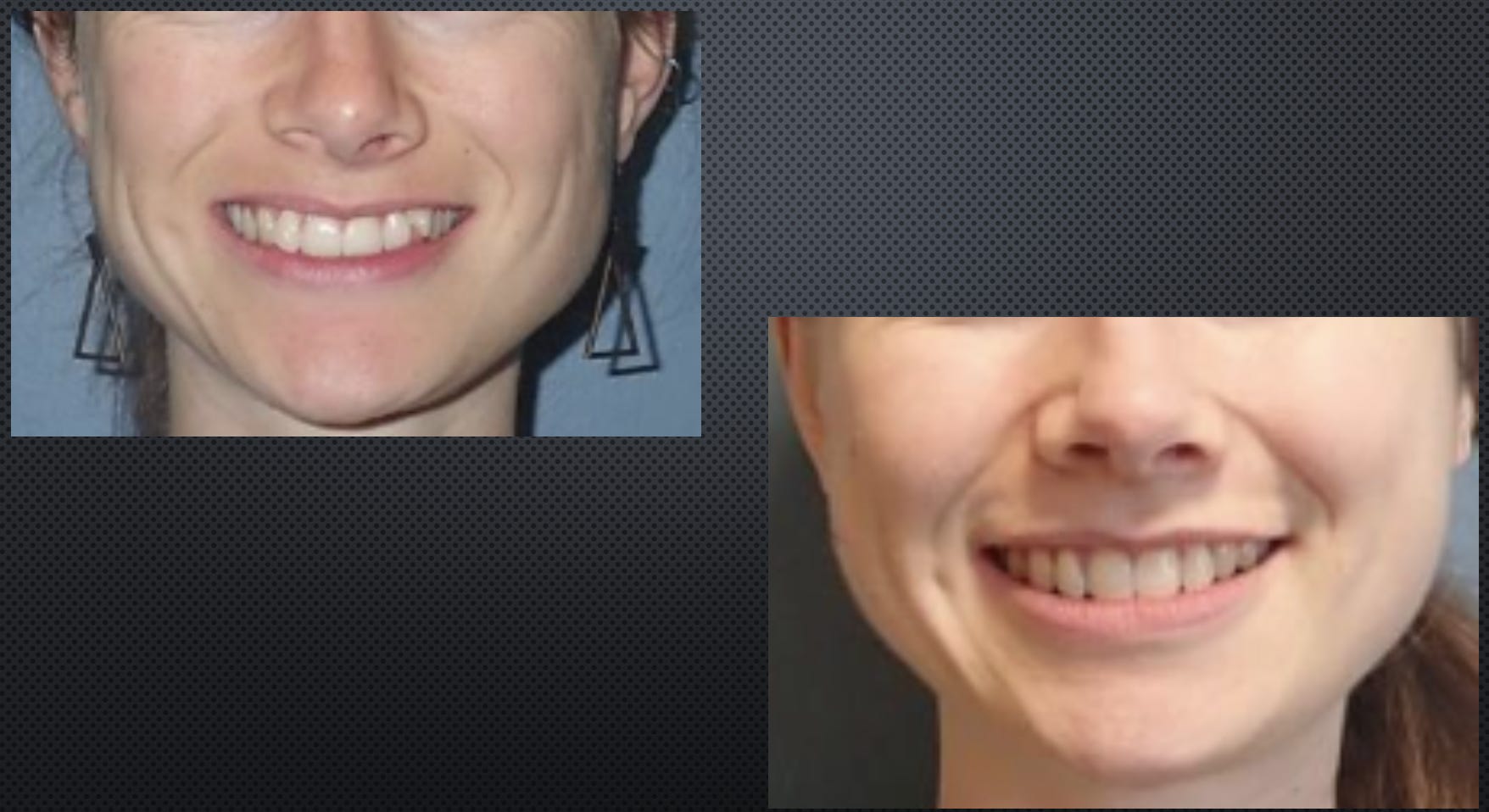
And you can see from the tone of the masseters, this patient’s primary concern was that of a clenching. Expanding the maxilla was, indirectly, the tool that we used to help provide more of a house for the mandible and the lower teeth, and resolve the lower crowding and upper crowding at the same time.
Expansion with Protraction – “Good Alone, Better Together”
Many of you know we’ve talked about the value of protraction. And I think, actually, protraction and forward movement of the jaw has the potential to be most transformational.
I think having increased access to expansion for all ages has been extremely transformational. But I think what will be more transformation is actually when we as community figure out protraction of all ages.
See the Potential Goodness in Your Face
This is a quick reminder to the youngsters out there watching, perhaps not limited youngsters, who may be so fixated and worried about the downstream effects of their suboptimal facial structure that they also fail to see some positives within it, or perhaps some of the opportunity for this to easily switch and go positive.
We as a community have grown good at pointing out shortcomings in people’s structures. But it’s also important to point out merits in people’s structures as it pertains to overall well being. We’re not only “structural improvement” doctors and functional doctors, but we are doctors of mental and emotional well being as well when you do this kind of work.
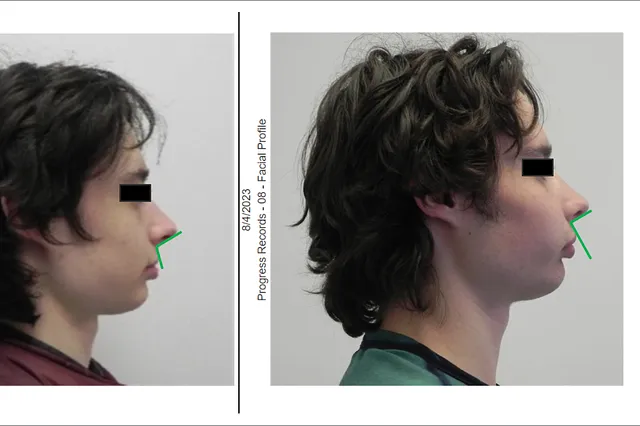
Comments on Scolopendra Case
Some of you who frequent certain talk spaces may recognize this individual. This is a very good case to show the facial effects of protraction orthodontics in adults — that it’s indeed possible. This person expanded beyond a level that was customary, and beyond what I would have customarily allowed.
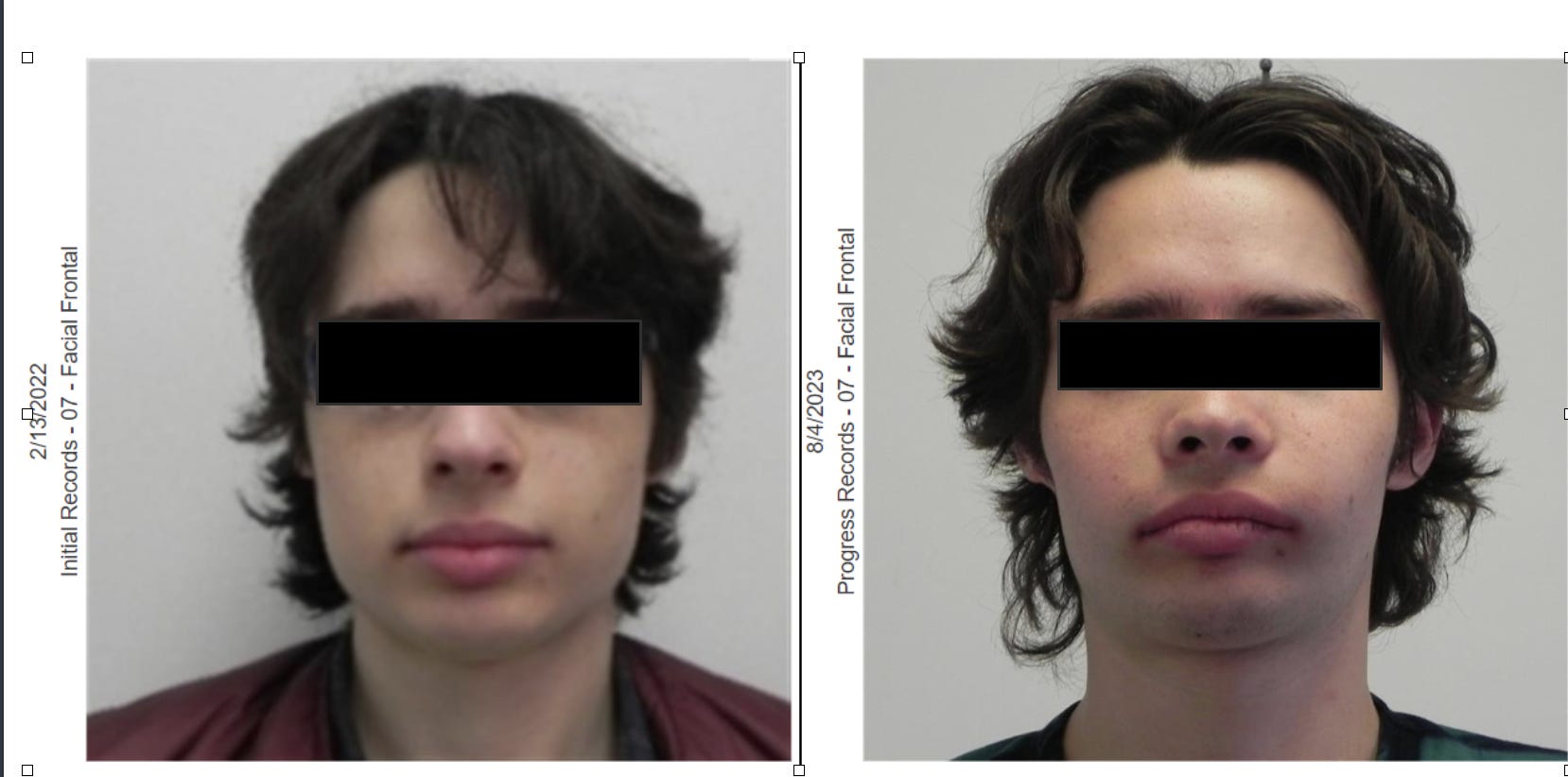
But we had a few unique things. There was some lax facial soft tissue and it took a large amount of expansion to fill out his buccal corridors. And I’ve been reprimanded on some of these talk spaces for allowing the patient to do this.
But me and the patient alike saw a pathway to be able to put this back together—because, of course, the lower jaw now is looking like it belongs to a different person. This is work in progress.
The lower jaw — we had a good presentation today by Ronny [Ead] that shows us that we have a lot of possibilities for enhancing mandibular structure and function. And basically it took a degree of fearlessness and mutual trust for us to pull this off.
But as a result, even though he has very little functional coordination right now, he is very happy with the amount of expansion and protraction he got. He almost got a Lefort 2 or 3 style protraction because of how profoundly his midface came forward.
So this is, again, is just to show the possibilities. This is non-surgical bone anchored protraction. This is not upper jaw surgery.
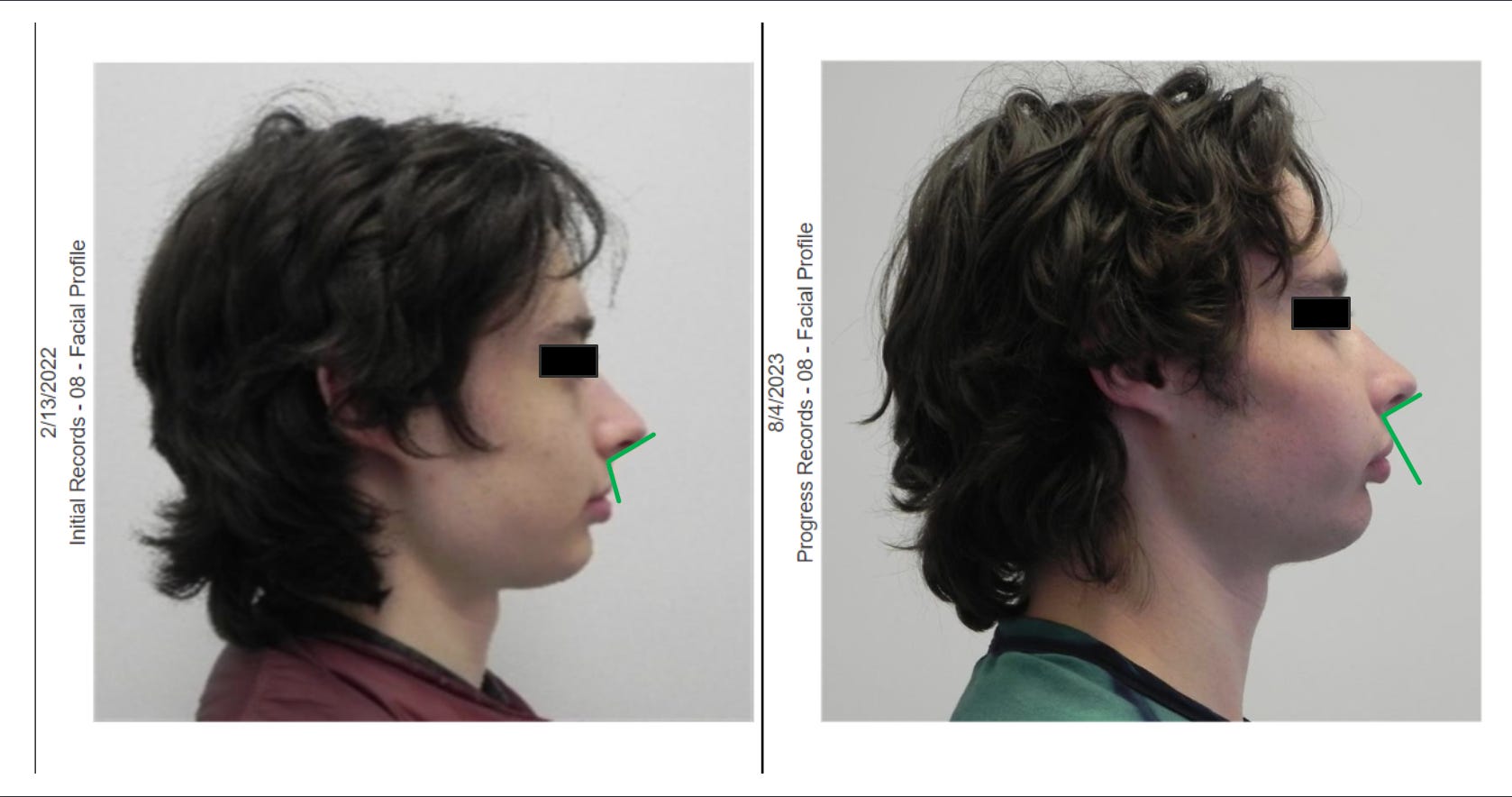
But you can see how obtuse that nasolabial angle was pre treatment. And then you can see that it’s about a right angle, or maybe slightly acute, after.
This patient actually very compliantly, religiously wore the bow designed by Dr. [Sandra] Kahn, especially in the height of his suture loosening. He’s been a model for being able to show that the adult protraction does indeed work. And he’s not the only one. I think you’ll find a lot of other evidence online that this is actually a thing.
Next Post
Next week, we will cover more of Dr. Newaz’s MewCon talk, which includes a discussion of the Rise of Custom MARPE, a technical explanation of the Facegenics Midface Expander (FME), and more.

