Below is a lightly edited transcript from the second half of the talk by Dr. Zubad Newaz, DDS at MewCon 2024 on August 17. All images shown below are from Dr. Newaz’s MewCon 2024 slideshow.
The Rise of Custom MARPE
All the patients shown so far have been treated with what we now view as perhaps a more primitive form of an expander device [in reference to MSE type 2, see previous week’s post]. They have worked well for younger people and females.
But now…we didn’t used to be able to look at somebody in the face, if you’re a 40 year old male, you come to the office, you’re seeking skeletal expansion. I couldn’t really look at somebody straight in the eye and say “we will be able to expand your palate.”
But with the advent of custom MARPE, where we can superimpose surface data with a 3D scan and be able to identify which parts of the bone and where exactly and how we want to place the expander’s anchorage. It was game changer.
And this was also a game changer because now I’m not stuck with a particular predetermined orientation of a pre-fabricated expander.

CBCT Planning of Custom MARPE
So the 3D guided MARPE fabrication relies on your CBCT scan planning, the placement of the screws, and we instruct the lab on a lot of different parameters in this kind of case, such as location and number of the lumens (the little holes for the screws). We have as much control as we want on that issue.
Also, accessory arms.
It helps to have a workflow where we can adapt the underside of the expander body to a patient’s individual anatomy. That is what has made custom MARPE be our staple tool for predictable adult expansion.
But it does have its drawbacks. Expansion as it exists in 2024 is not perfect, but it has been a very good tool to help people of all ages gain real estate in their mouth, nasal breathing and so forth.
Armless MARPEs?
We can instruct the lab on accessory arms. Where do we want, or not want, tooth anchorage. We do toothless versions of these all the time as well, where we will make it with an armed framework to seat it predictably as planned, and then immediately proceed to cut the arms off so that the expander is toothless.
You may do this for an individual where you really are concerned about or want to minimize, to the best degree possible, any sort of unwanted flaring or periodontal effect on the teeth.
Even though we anticipate the expansion to be mostly coming skeletally, it doesn’t always end up being 100% skeletal, that’s just the honest truth of the matter. Anyone who tells you otherwise is not being totally honest.
And that’s okay. It’s okay to have a little bit of hybrid-style expansion, as long as you know what you’re getting, how you’re doing it, how to see what you’re getting, and how to see whether that’s appropriate for the individual patient.
Arms for Intrusion, Protraction
Then, of course, it’s easy to put on whatever accessory arms or whatever you want for protraction or intrusion.
Intrusion is a very common thing that we end up using with bone anchored expansion, because it is what allows the lower jaw to auto rotate into a more forward position after you have gotten some of the natural forward outward rotation of the maxilla as a result of doing this style expansion, where expansion tends to pivot about this *points to zygomatico temporal region*.
So we have these trinkets that we can put on our expanders for a number of select applications.
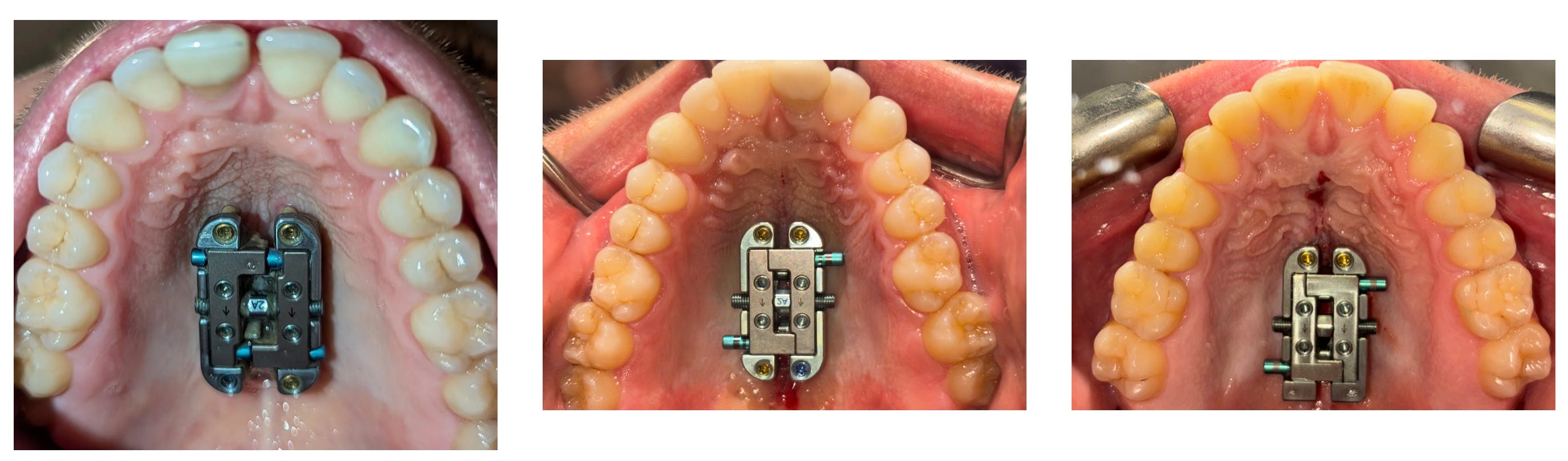
Intro to FME
This is another expander that we use now, and as of just a few weeks ago we were the only practice doing this. It is the Facegenics Midface Expander (FME).

Dimensional Stability of FME
Basically what this is, is an evolution from some of what we have now learned are shortcomings in the dimensional-stability-forgiveness built into other kinds of expanders.
We have all learned now that bone anchored expansion comes with its drawbacks. Asymmetry is the biggest drawback. Lack of dimensional stability of the expander body is a big drawback.
I talked to another participant here today, where we shared the experience where sometimes you’re cranking that MARPE screw, and then enough tension will build up into the device, even if the palate splits that you can’t turn the screw, it kind of gets stuck.
Why would that happen in a mechanism where you have a telescoping barrel, where things are supposed to come out of each other in parallel. Well, something must not be parallel if it’s getting stuck right?
Locking TADs
This particular team of individuals (Faccgenics) who started this company, they’ve been working on this expander for a long time to try to overcome some of these physics challenges that exist with bone anchored expansion, to make the expander body as unforgiving to twisting/rotational/shearing forces as possible.
And one of the ways that they’ve been able to do that is to lock the TADs into the body of the expander where there’s zero play between the screw in the palate and the expander body.
Being able to do that at least confers some level of predictability of the dimensionality and direction of your expansion.
But this is super early. We don’t know if, for example…maybe, between the screw and the screw housing, we have a perfect relationship — but maybe between the screw and the native bone, we don’t have a perfect relationship. We have to see what the effect of that is going to be as far as this appliance’s propensity to drift or rotate.
We have to now see if [the FME] performs a little better than other things we’ve had in our hands these past few years.
The field of bone anchored expansion is rapidly changing and evolving, so we’re trying to stay with it.
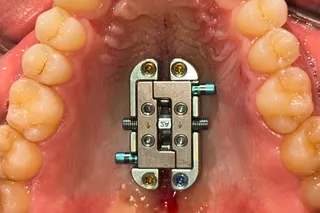
Detachability of FME
What you just saw in the prior slide [above] was a 6 screw version of FME. It has 4 holes on the top, but those actually are not the screws that go into the palate. Those are the screws that lock the expander module onto the little plates that connect to the palate.
And having it be detachable is good, because you can reload your expansion without reinstalling the whole thing.
You can also dismount the expander if you have a clinical problem beneath your expander. With other expanders, right now say you have an oronasal fistula, a bone problem in the center palate, you can’t necessarily see or access that.
But with FME I can just take this top piece off so that the clinical condition underneath the expander can be evaluated.
So I think that this has been also a nice upgrade into the world expansion.
FME vs. Custom MARPE
I say “upgrade” not to mean that FME is categorically the best expander, but rather to say that is has the potential to overcome some of the limitations [of other expanders].
But I still find that custom MARPE is perhaps a bit more predictable, at least in my hands today, since I have only installed 9 or 10 FMEs.
Also, some of the characteristics of custom MARPE are better for some individuals for whom we may need to work with irregularities in the native anatomy.
“Composite Bone Anchorage”
FME fabrication is in large part very similar to custom MARPE. It depends on the use of surface and 3-dimensional imaging data radiographically to plan the positioning of the appliance to maximize your composite bone anchorage.
“Composite bone anchorage” is a word I like to use to describe the fact that the success of adult bone anchored expansion is directly proportional to this composite bone anchorage — putting 6, 8, 10, whatever amount of screws we’re putting in, we need a high quality screw to bone interface, and we need it well-spread out across an axis that will allow for a dimensionally favorable expansion.
So all of that is the phenomenon I call composite bone anchorage.
FME Installation
This is some of the process of delivering the FME, where everything is surgically guided.

We don’t have any tooth attachments [with FME], so how do we deliver it in a predictable position, exactly where we planned it?
It’s using these guides.
We put the plates that are going to house that expander and actually screw it into the guide so it doesn’t move when you’re bolting it in.
FME Fabrication and Key Points
- Impression of upper arch with whole palate
- CBCT scan
- Locking TADs
- Rigid expander body
- Detachable expander
- Anchor plates placed first with TADs then expander mounted on
- Titanium construction
- Does not tolerate bending and twisting forces
- Armless
- Surgically guided installation

