
MSE: 1 Week, 20 Turns, Suture Split
This post documents my first week with MSE. It was tough, but by the end of it I had achieved a successful split of the mid-palatal suture.
On July 15, 2019 Dr. Zubad Newaz, an orthodontist at the Gelb Center in Manhattan, performed a cortical puncture on my mid-palatal suture and installed the maxillary skeletal expander (MSE).
A view of my Maxillary Skeletal Expander (MSE)
MSE Install Pain - 3 Tough Days
I experienced significant amounts of pain for three days after the install. During those 3 days I did not turn the appliance, as introducing tension increased the pain and triggered headaches.
Before treatment I was aware that MSE would be fairly invasive, as it involves bolting four 11mm screws into the maxilla (not to mention cranking the appliance with the intention of splitting the maxilla in two).
Also, the cortical puncturing involves drilling holes in the suture which is quite invasive too.
But I successfully avoided thinking too much about the potential pain leading up to the procedure, so as not to scare myself out of doing it.
Well, I must say that for 3 days, the pain was just as bad as you might expect.
The procedure itself was mostly painless, no worse than having a cavity drilled and filled. This is because copious amounts of local anesthetic is injected into the maxilla and you are totally numb to the corticotomy and the bolting of the screws.
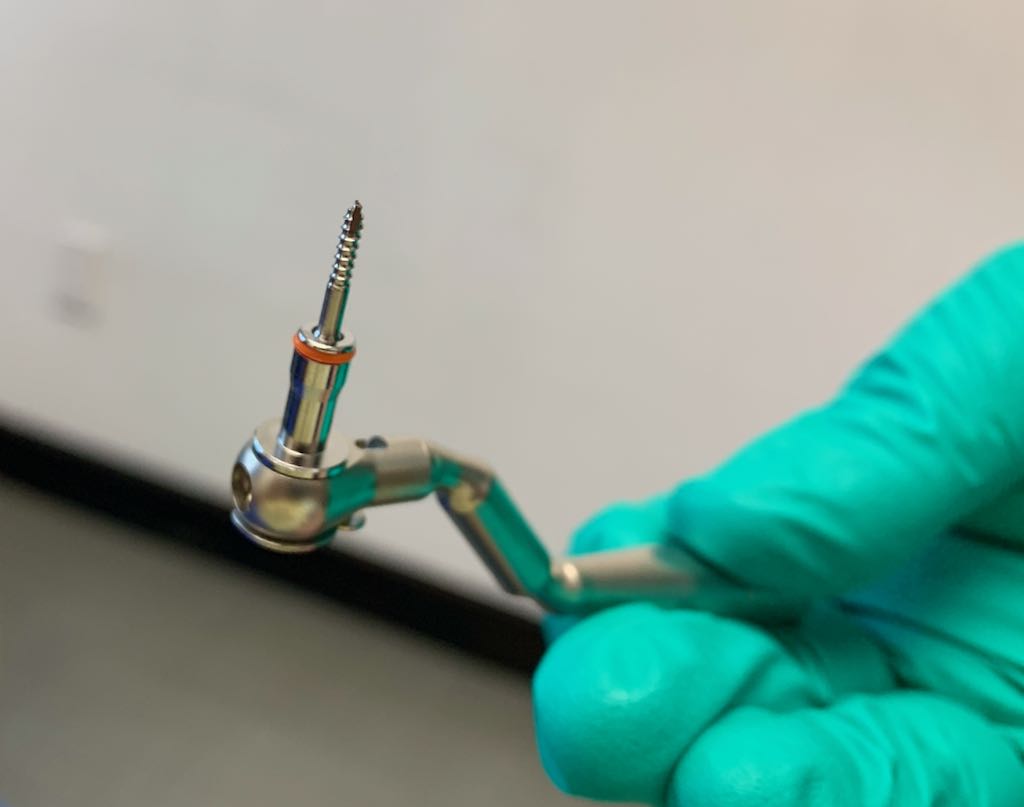
Dr. Newaz holding one of four 11mm screws placed in the maxilla as part of MSE install. Long screws are necessary in order for the MSE to transfer its splitting force to as much maxillary bone as possible, so that it can win its battle with the mid-palatal suture.
But suddenly, just about 3 hours after the placement of the final screw, the novocaine wore off and the pain hit me like a brick wall. Thankfully my father was there to drive us up from New York to Boston.
Dr. Newaz said that it was not typical for patients to experience as much pain as I did. I believe that my genetic proclivity to experience migraines made my MSE install significantly worse than for the average patient.
I say this because the worst aspect of the pain I experience after the MSE install was severe headaches.
Yes, there was definitely dull, throbbing, even stabbing pain in the maxilla itself resulting from the punctures and screws. But what made these 3 days so tough was the overwhelming headache pain that set in.
Most likely this is not a common experience and Dr. Newaz confirmed as much. But anyone with a chronic headache condition may want to plan for MSE to trigger some episodes.
As a migraineur, I think of my body as having several smoke detectors, spread out and connected in series. The way smoke detectors work is that when one is triggered, they all go off.
I think MSE set off a smoke detector in my body, and the result of that was that my entire body went haywire with headache.
For 3 days I was somewhat incapacitated, as if I were recovering from a small surgery. I did successfully do a 2.5 hour physics lab and take a tough 2 hour exam less than 48 hours after install, so I wasn’t totally knocked out.
I managed the pain with triptans, Tylenol, and a microwavable rice-sack that I wrapped around my face, head and neck. I also self-massaged frequently with a Theracane.
During these first three days, I attempted to turn the MSE’s screw on several occasions. But whenever I did, the pain became much worse and I turned the screw back to zero, and experienced immediate relief.
Then the Pain Suddenly Vanished
On the Thursday afternoon after the Monday MSE install, my body suddenly chilled out. The smoke detectors went silent.
For whatever reason, my body decided to accept the fact that 4 large screws had gone into my skull, and holes drilled too, and reset itself to a pain-free homeostasis.
Eager to take advantage of the still-fresh cortical punctures, I immediately seized the opportunity to start cranking the appliance. (The punctures would heal and solidify soon, reducing my odds of splitting the suture).
I turned the screw once and immediately felt the headache pain setting in. To calm my body down, I went over to my oxygen tank (I keep a tank of pure welder’s oxygen in my room and occasionally huff oxygen in order to abort headaches), and did about 5 minutes of deep oxygen breathing.
My body calmed back down.
This is the technique I would use to get me through the next 3 days of aggressive turning: I would turn the MSE screw, and then huff oxygen for 5 minutes until my body chilled out.
Combined with the hot rice sack and Tylenol, I was able to turn the screw 7 times that Thursday, without headache.
On Friday I kept the rhythm going – 6 more turns (2 in the morning, 2 in the afternoon, 2 in the evening, with 5 minutes of oxygen after each turn).
On the third day, at turn 20 or so, I felt my suture split.
I knew the suture had split because after turning the screw several times and introducing high amounts of tension, all of a sudden I felt a warm sensation shoot across my suture.
This shooting sensation was followed by a drastic release in tension in my jaws and midface.
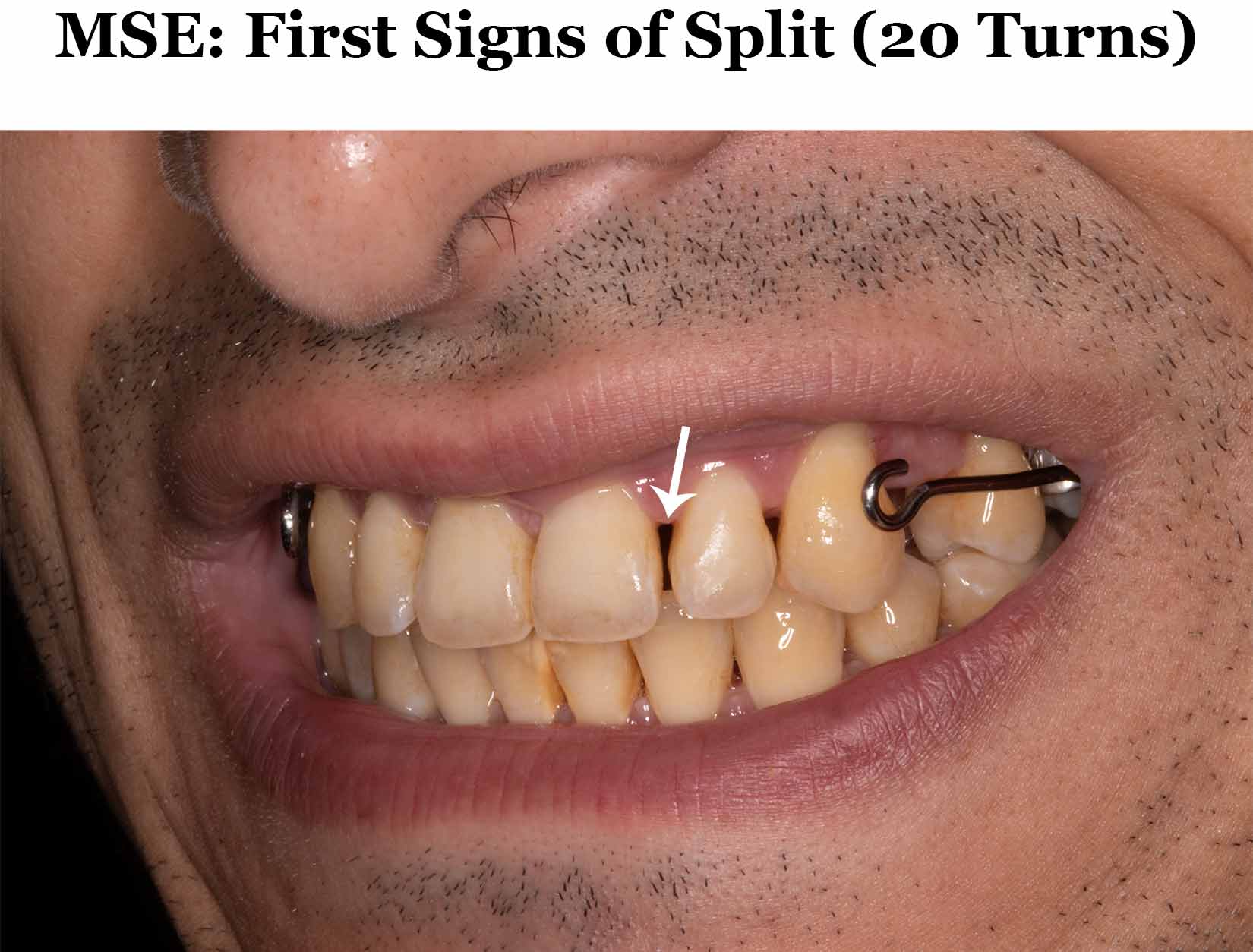
When I looked in the mirror, I noticed that gaps had formed, but not between my two front teeth as I expected. Instead, the gaps formed between teeth 7-8 and 9-10, as shown in the images below.
These images were taken the day I felt the suture split.

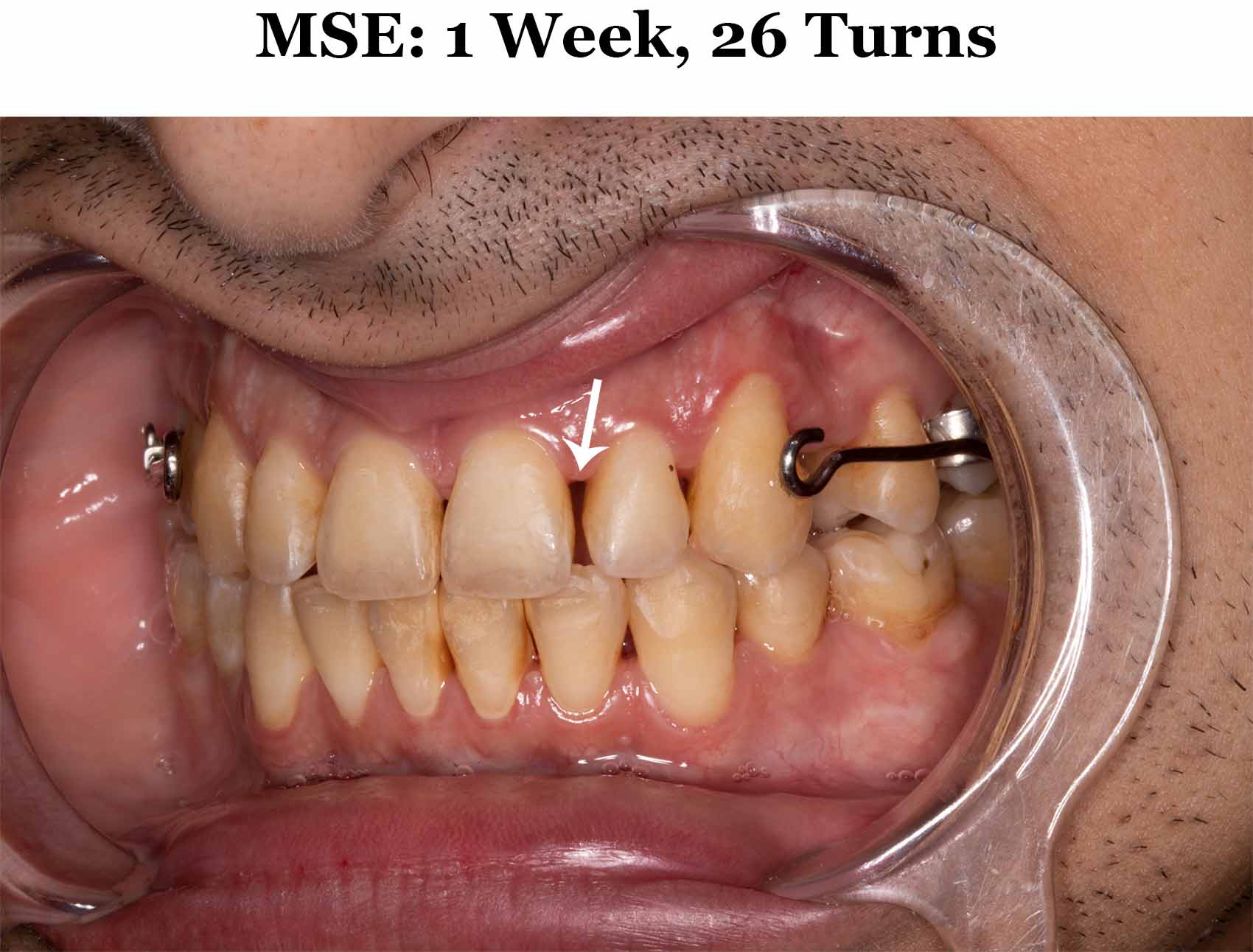
The day after the split, I turned the MSE 6 more times. Even though you are only supposed to turn a maximum of once per day after the split occurs, I felt like I wanted to deal the suture a death blow and be certain that I was over the hump.
After those 6 turns, a distinct diastema appeared between my two front teeth as shown in the images below. The gaps between teeth 7-8 and 9-10 remained.



It’s All Downhill After the Split
After the split occurred, I reduced my rate of turning to 1 turn per day.
At this point, tension/pain throughout the skull caused by the appliance was greatly reduced. The severe tension in the maxilla, cheeks and nose was almost completely eliminated.
Based on my experience with MSE, the process leading up to the split is definitely the worst part.
Once the mid-palatal suture is released, the great majority of craniofacial discomfort resulting from MSE screw-turning subsides.
The split is a major milestone, but one that for me required endurance, mental fortitude, and skillful pain management to achieve.