Ron gave this talk at the first ever MewCon in New York City on August 17, 2024.

Introduction: What is Airway Maximalism?
A big part of what I do is maintain a 12,000ft view of the airway world. Since I am purely a consultant, and do not offer any treatments of my own (since I am not a healthcare provider of any kind), I have the luxury of being able to keep a very broad, disinterested view of all airway treatments modalities.
In this talk, I want survey 5 approaches to maximizing three dimensional jaw augmentation that I am seeing done, and that clients regularly ask me to help them compare and contrast, in terms of pros and cons.
First of all, what do I mean by 3 dimensional jaw augmentation? By this, I mean both widening and advancing the jaws as much as is reasonably possible for a given patient. Think: make the box bigger, in every way.
3 dimensional jaw augmentation is something generally sought after by what I call “maximalists,” which are patients that want it all – the full monty of jaw reconstruction. As one client aptly put it when explaining his case to me last week: “I need everything,” he said.
This particular patient was a 36 year old army veteran with long brown hair and jaws so small and so recessed it looked like he had a permanent frown on his face. This man was worn thin, and desperate for air and for sleep.
To quote the TV show True Detective: I could see his soul bleeding out the edges of his tired eyes.
2 Types of Airway Maximalists
Generally I find that airway maximalists tend to fall into 2 categories: 1) desperate airway patients who are approaching death’s door, such as the man I just described and 2) bold biohackers who are doing pretty good but want to be doing great, and they have the money and the balls to try and make that happen.
These are the type of people who are willing to just “go for it,” doing extreme, unconventional things with their time and with their bodies in order to have great experiences in life.
A good example of the latter category is a client who I spoke to recently who was a 29 year old, wealthy digital nomad who spent almost 2 years on a waitlist to have a famous New York tattoo artist sleeve both his arms, and who called me from the Philipines where he was “geomaxxing” with a group of friends.
This means he proactively sought out a country where his American dollar was more valuable and his European appearance was rarer and more appreciated, in order to maximize his chance of dating success. Clearly this guy was a serial optimizer.
He had a visibly narrow palate and recessed jaws, wanted to solve his breathing troubles, fix his TMJ pain and, of course, look better. And he wanted to do it quickly and without compromise. He wanted a path forward that was fast and maximally effective, and his tolerance for more invasive procedures was high.
Foreshadowing: he was interested in the fastest, most invasive and most effective treatment to be discussed below. Option #5.
Perspective
Now, not every airway patient is a maximalist and I’m certainly not saying that they should be. But I’m also not going to stand in judgment of maximalists either, especially if they decide to pursue these treatments armed with full understanding of the potential risks, costs and pitfalls.
And if maximalism is not your particular interest, I think there is value in understanding the airway maximalist modalities.
Regarding the treatments to be discussed below – this is it. They are the final frontier of jaw augmentation, at least for now. You are about to reach the edge of the Milky Air-way Galaxy.
If nothing else, this discussion should give you perspective on where your own, more conservative approach to treatment falls on the full spectrum of all possible jaw augmentation modalities.
5 Approaches to Jaw and Airway Maximalism
And so, here are 5 paths of treatment presently being considered by many airway maximalists.
What all 5 paths have in common is that they are primarily bone-borne approaches, and whenever dental augmentation is used, it is used only as a complement. In other words, the bone-borne modality is the meat, and the tooth-borne expansion is the sauce.
OPTION 1 – MARPE + SFOT + Dental Expansion on Upper and Lower
The first treatment approach is MARPE + SFOT and Dental Expansion on the Upper and Lower. Of the 5 paths to 3 dimensional jaw maximalism that I will be discussing, this is the only one that does not include orthognathic surgery, although it does include SFOT which is a kind of surgery, and not a very pleasant one at that.
Dr. Joseph Yousefian in Bellevue, WA has an interesting take on MARPE + upper and lower SFOT. He calls it MAPES (Microimplant-Assisted Protraction Expansion Surgery).
It involves a MARPE with arms that extend forward and attach onto the 6 upper front teeth. Those arms have their own jack screws, one on each side, and those screws can be turned to push the upper front teeth forward using the MARPE as an anchor.
With the support of SFOT, this anteriorizing of the upper front teeth is relatively safe as compared to toothborne expanders like AGGA. And with anchorage to the MARPE, you don’t get the upper molars being pushed back at all due to Newton’s 3rd Law such as we saw with AGGA.
And with the support of SFOT on the bottom, dental expansion can be used to get the lower arch to match the upper in all dimensions.

All things considered, this is about as good as it gets for 3D jaw augmentation for those that are dead set against the Lefort and BSSO cuts that come with orthognathic surgery. Although of course the magnitude of advancement that can be achieved with MAPES and SFOT is not in the same league as that which can be achieved with a true jaw surgery.
OPTION 2 – MARPE + Facemask + Lower Jaw Surgery
The second treatment approach to 3-dimensional jaw maximalism is MARPE + facemask + a lower jaw only surgery. I will call this approach theoretical for now since I don’t know anyone who has actually done this.
This approach involves a MARPE to widen the upper palate, and to loosen the various sutures of the face, which paves the way for a protraction device. With enough compliance, the facemask can be used to pull the maxilla and entire midface forward, far ahead of the mandible. Which then forces the patient into a situation where the mandible needs to be augmented to match.

Sure, dental expansion could be used to buy you a few mm of anteriorization of the mandibular teeth, but that approach would set very underwhelming limits on how far the patient could go with the facemask.
However with a lower jaw surgical advancement, the facemask could be used to its full potential.
This would allow the patient to avoid the scary Lefort cut on the upper jaw, and potentially pull the entire midface forward rather that just than just the maxilla, as occurs with even a high Lefort cut.
Although disadvantages to this approach include 1) its dependency on patient compliance with the facemask, which many find to be miserable, 2) inability to have a predictable rotational upswing of the jaws, also known as counterclockwise rotation, with the facemask, and 3) the potential for post-surgical numbness, which is almost always worse on the lower jaw, which is the jaw which would be operated on in this approach.

It would take a very special kind of patient to attempt this approach – notably, one who is very curious and interested in experimenting with a facemask

OPTION 3 – MARPE + 1 Piece Maxilla and 1 Piece Mandibular Surgery
A third approach to 3 dimensional jaw maximalism is MARPE followed by a simple, standard one piece upper and one piece lower jaw surgery.
This approach is great for those who aren’t sure if they are true maximalists, because they have the option to bow out of the jaw surgery if the MARPE gets them what they’re looking for.
That could mean enough nasal breathing improvement and tongue space to go on living. Or maybe from an aesthetic point of view, they are happy to have a wider, more Hollywood smile, and sharper cheekbones, and can do without the killer side profile.
But if they feel like the MARPE wasn’t enough, and they still want the surgical advancement, now they can take a simplified approach to surgery by doing a 1 piece upper jaw surgery, which is simpler, harder to botch, and has less risk to the health of the teeth. Also a lower infection risk as it means less surgical plates, which are often the site of post-surgical infection. A once piece upper jaw surgery is also a faster surgery, which means less tissue jostling, less anesthesia, etc. which translates to an easier recovery.
Finally the last advantage of this approach, and perhaps the most important, is that the MARPE may give certain nasal breathing benefits that orthognathic surgery simply cannot.
Specifically, it can expand the nasal volume vertically along the y-axis of the nose, because the it spreads the nose basically all the way up to the base of the eyes, as opposed to jaw surgery which only expands the nose up to the height of the Lefort cut.
Higher Lefort cuts as part of a segmental Lefort may approach the effectiveness of the MARPE in achieving nasal volume expansion up the vertical axis of the nose. But patients who present with distinctly poor nasal breathing should strongly consider this benefit of MARPE when weighing their treatment options.
OPTION 4 – 3 Piece Maxilla, 1 Piece Mandibular Surgery + SFOT
The fourth approach to 3D jaw maximalism skips MARPE altogether. It involves a 3 piece maxillary segmental osteotomy to both advance and widen the upper jaw, a BSSO to advance the lower jaw, and later SFOT and dental expansion to widen the lower arch.
This approach hinges on the fact that orthognathic surgeons are quite proficient in doing multi-piece upper jaw surgeries, to both widen and advance the upper jaw. Most of them offer this as an option.
But multi-piece lower jaw surgeries are much rarer, which means dental expansion is still needed to get the lower jaw to match.
This MARPE-less approach appeals to those interested in speed and efficiency, as they can get a MARPE-like result without going through a multi-year orthodontic process.
For example, many patients have bites that suit a surgery-first approach that allows them to go into surgery immediately without doing any preparatory orthodontics.
So why would they seek out a MARPE, with its cost, known risk of asymmetry, difficulty in splitting adult males (which, of course, often requires its own surgery), and two years of associated orthodontics, when they could go into surgery tomorrow and get an arguably more precise, more predictable expansion in 3 hours?
Sure, the segmental Lefort does not provide the desirable zygomatic enhancement that MARPE does, since the lever arm of the expansion is severed at the site of the Lefort cuts, beneath the zygomas. Although this can be ameliorated with malar implants, such as those done by Dr. Gunson.
And as mentioned before, theoretically, MARPE does have the potential to expand more of the nose, up the y-axis.
But are these reasons enough to warrant the time and hassle of MARPE? More and more patients are asking this question.
OPTION 5 – 3 Piece Maxilla, 5 Piece Mandibular Surgery
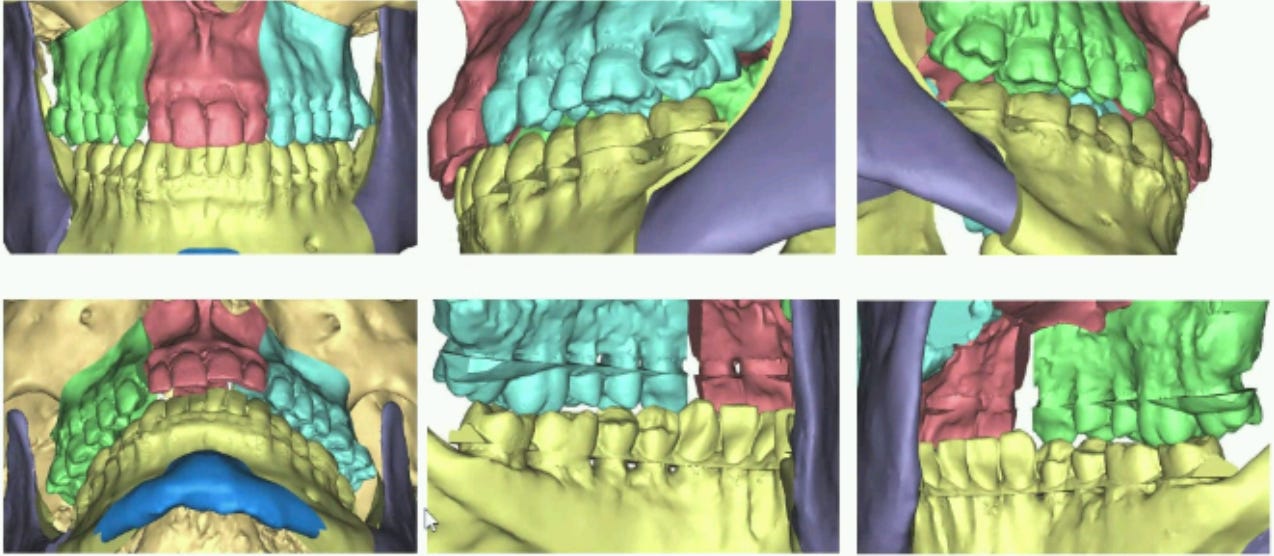
The fifth and final approach to 3D jaw maximalism that I will discuss today is a 3 or 4 piece segmental maxillary surgery combined with a multi-piece mandibular surgery, such as Dr. David Bell’s 5 or 6 piece mandibular surgeries. Other surgeons do this too, but not many.
This is complete and total reconstruction of both jaws in one day. Widening, advancing, re-angling. The whole, 3-dimensional shebang.
Specifically what is unique about this approach is the mandibular skeletal widening. The type of widening that Dr. Bell performs is not at all like a mandibular midline distraction, also known as MSDO. MSDO widens the front of the jaw, but does not widen the proximal segments, which are the back of the jaw, at all.
Shuikai has argued that MSDO is an unnatural kind of mandibular widening that has very limited airway and aesthetic benefits if at all, along with a greater risk of TMJ complications.
But Dr. Bell’s manner of expanding more closely mimics natural mandibular growth. He widens and arranges the proximal segments in a manner that produces better aesthetic and airway outcomes, and without stressing the TMJs.
Of course the downside of this approach is the recovery. That’s a lot of bone cutting and a lot of plating. And more plates means increased risk of infection. Soft tissue draping into the site of the bone gaps can also be an issue.
But if you could wave a magic wand over your own head and wake up 6 months after a surgery like this, and having had it all go well, that would be some result, wouldn’t it?
So, now that we have reviewed 5 approaches to 3D jaw maximalism, I will leave you with one question: who’s ready to have their jaw cut into 9 pieces?
Thanks!


